

RDAs Explained: Why the "Recommended" Daily Allowance Is Keeping You Sick
- templefoods9
- Apr 14
- 13 min read
The Minimum Legal Standard for Not Being Dead
Here's something worth knowing about ice cream in South Africa: there are minimum legal standards to call a product "ice cream." The product must contain at least 6% fat and a minimum proportion of milk solids. Below that threshold it legally cannot be called ice cream - it must be labelled "frozen dessert" or "dairy blend" or something equally uninspiring.
Meeting those minimum standards doesn't make it good ice cream. It makes it legally ice cream. You can still make it with the cheapest ingredients, fill it with stabilisers and gum, load it with sugar, and produce something technically qualifying while no reasonable person would call it food worth eating.
The Recommended Daily Allowance - RDA, or NRV (Nutrient Reference Value) in South African regulatory language - is the nutritional equivalent of that minimum legal standard. It is the floor below which you officially become deficient. It is not the amount that makes you thrive. It is not the amount a high-performing body needs. It is the amount required to call yourself "not deficient."
And this distinction - between "not deficient" and "optimal" - is the gap that the entire supplement industry, the pharmaceutical industry, the food industry, and the regulatory bodies would prefer you didn't think too hard about. This article is about that gap.
What Is an RDA, Exactly?
The RDA was developed in the 1940s, primarily to prevent deficiency diseases in wartime populations. The central question being answered was not: How much vitamin D does a person need to have excellent bone density, robust immune function, and healthy cognitive performance? The question was: What is the minimum amount to prevent rickets?
This is the foundational problem at the heart of nutritional medicine. The RDA was designed to answer the wrong question - and it has been used ever since to reassure people that if they're hitting these minimums, they're fine.
They are not fine. They are just not dying of a classic deficiency disease. There is a vast stretch of health territory between "alive and not acutely deficient" and "optimal." The RDA marks the entry to that territory. It doesn't tell you anything about what's on the other side.
Consider vitamin D3. The current international RDA is 600 IU for adults. This is the amount required to prevent rickets in children and osteomalacia in adults. Meanwhile, the Endocrine Society has stated that pharmacological doses up to 10,000 IU daily are safe for long-term use. Peer-reviewed research associates optimal immune function, cancer risk reduction, and cardiovascular health with serum levels that require 5,000–10,000 IU daily supplementation for most adults living indoor lifestyles.
The gap between 600 IU and 5,000 IU is not a minor rounding difference. It is an 8-fold gap. This is the gap the RDA framework tells you doesn't matter. It does matter.
Who Sets the RDAs? (And Who Pays Them?)
If you want to understand why the RDA system has not changed significantly in seventy years despite mountains of contradicting research, follow the money.
The 2020 US Dietary Guidelines Advisory Committee - the body that recommends what Americans (and by extension, the world) should eat - was composed of experts, 95% of whom had documented conflicts of interest with the food and pharmaceutical industries. This is not a claim. It was published in peer-reviewed literature: Mialon and Swinburn (2020), PLOS Medicine, PMC10966930.
Think about what that means structurally. The committee that sets the guidelines determining what is "sufficient" and what is "deficient" is populated almost entirely by people with financial relationships to the companies that profit from people staying at the minimum rather than the optimal.
There is no conspiracy required here. No secret meetings. Just standard institutional capture: if the cardiologist on the committee has a consulting relationship with a pharmaceutical company that makes statins, they are structurally incentivised to set lipid thresholds in ways that maximise statin prescriptions. If the nutrition expert has relationships with the sugar industry, they are structurally incentivised not to set sugar toxicity thresholds too low.
We don't have healthcare. We have sick care. If you're not sick by the clinical definition — which is built on RDA-based thresholds — you're "healthy." And if you're healthy, you don't need medicine. The system works perfectly for everyone except the person whose health is being managed.
The SAHPRA Problem: When Minimums Become Maximums
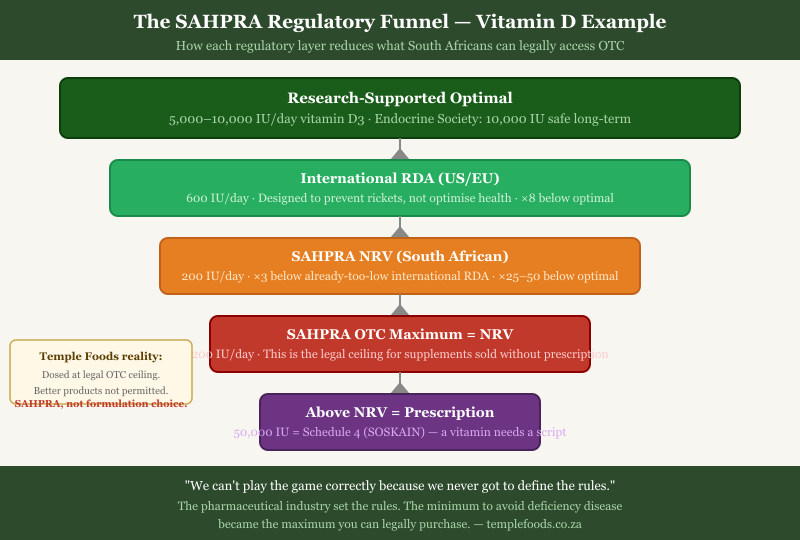
In South Africa, the situation is not just broken — it is inverted. SAHPRA (the South African Health Products Regulatory Authority) has taken the NRV framework and done something uniquely destructive with it: they use NRVs as maximum allowed dosages in over-the-counter supplements.
Read that again. The minimum amount required to not be officially deficient has become the maximum amount you are legally allowed to purchase without a prescription.
The South African NRV for vitamin D is 1000 IU. That is the OTC ceiling. If you want to purchase vitamin D at 50,000 IU — a therapeutic dose used clinically to correct severe deficiency — you need a prescription for SOSKAIN, a Schedule 4 medicine. A vitamin requires a prescription because it exceeds a regulatory minimum that was never designed to represent optimal dosing.
I want to be completely honest with you about what this means for Temple Foods products. Our D3+K2 formulation is dosed at the legal maximum SAHPRA allows for OTC sale. That maximum is still well below what the research supports as optimal. I would make a significantly better product if SAHPRA allowed it. They don't.
There are no better products available on the South African OTC market — not because of quality differences between brands, but because higher doses are illegal for OTC sale. Products exceeding NRV-based limits are removed from the market. The system is closed.
If you want to approach the doses that peer-reviewed research actually supports for optimal D3 levels, the legal mechanism within the SAHPRA system is to take multiple capsules. More costly. Inconvenient. But the only legal path until the regulatory framework is revised.
This is the honest reality: the game has been rigged. We can't play it correctly because we never got to define the rules. The pharmaceutical industry set the rules — and they set them to ensure that the most effective, cheapest interventions remain just below the threshold of clinical medicine, while keeping people just sick enough to need the expensive interventions that the same industry provides.
The Chain Problem: Why Isolated Studies Mislead You
There is another layer to this that the RDA framework doesn't just ignore — it actively obscures. The human body does not use nutrients in isolation. Vitamins and minerals are co-factors in biochemical pathways that involve dozens of nutrients simultaneously. Studying them one at a time, setting individual RDAs for each, and treating them as independent variables is biologically illiterate.
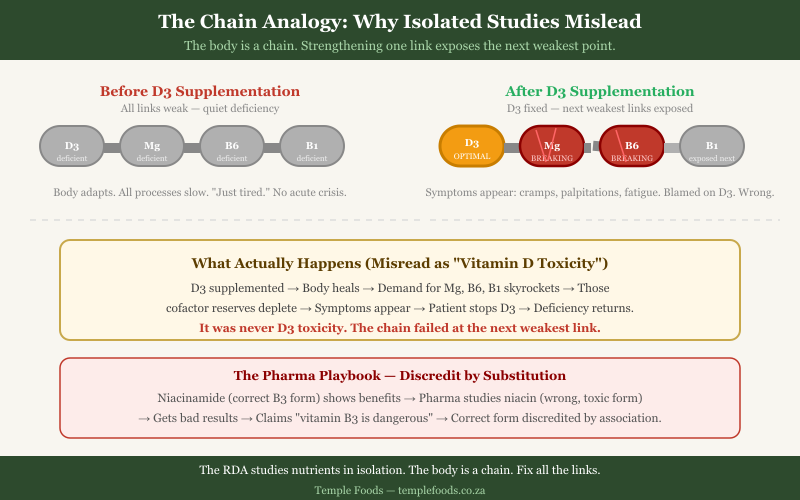
Think of the body as a chain. Each link is a nutrient. The chain fails at the weakest link. You can have the strongest D3 link in history, and the chain still fails at magnesium.
Here is how this plays out in practice — and why thousands of people report what they believe is "vitamin D toxicity."
A person is severely D3 deficient. They supplement at 5,000 or 10,000 IU daily. Their body begins to heal. Calcium metabolism improves. Immune function activates. Cellular repair accelerates. All of this requires co-factors: magnesium (for converting D3 to its active form), vitamin B6 (for dozens of downstream processes now firing correctly), vitamin B1 (for the sudden increase in energy metabolism).
As D3 finally works correctly, the body's demand for these co-factors skyrockets. If the person was borderline deficient in magnesium and B6 before — which most South Africans are — they now tip into symptomatic deficiency. They get muscle cramps, palpitations, anxiety, fatigue, brain fog.
They blame the vitamin D. They tell their doctor they had a "reaction" to D3. The doctor agrees. The supplement gets stopped. The root-cause D3 deficiency returns. And the medical establishment adds another anecdote to the file of "evidence" that high-dose vitamin D is dangerous.
It was never D3 toxicity. It was the chain breaking at the next weakest link, exposed only because D3 was finally making the body work hard enough to demand everything downstream.
The pharmaceutical industry has refined this playbook. Studies show niacinamide (the correct form of vitamin B3) helps with cholesterol and cognition. Pharma runs counter-studies using niacin (a different, flush-inducing, high-dose-toxic form). Gets bad results. Claims "vitamin B3 is dangerous." The correct form gets discredited by deliberate association with the wrong form. Brilliant, if your goal is to protect pharmaceutical market share. Destructive, if your goal is public health.
The Risk-Benefit Calculation They Don't Want You to Run
Let's apply actual numbers to vitamin D, because this is where the "safety" argument for RDA compliance collapses completely.
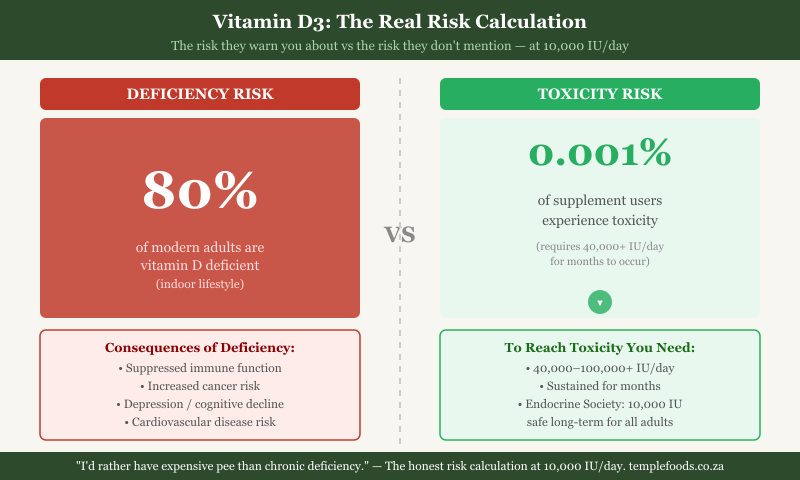
Vitamin D deficiency affects approximately 80% of modern adults living indoor lifestyles. The symptoms of deficiency include suppressed immune function, increased cancer risk, depression, cognitive decline, poor bone density, cardiovascular risk, and autoimmune vulnerability. These are not theoretical associations — they are documented in longitudinal studies across multiple populations.
Vitamin D toxicity — hypercalcaemia caused by excessive D3 — occurs in approximately 0.001% of supplement users, and only with sustained use of 40,000+ IU daily for months. The Endocrine Society formally states that 10,000 IU daily is safe for long-term use in adults.
The risk-benefit calculation is straightforward: take 10,000 IU daily, eliminate an 80% deficiency risk, accept a functionally zero toxicity risk at that dose. The people promoting the 600 IU RDA are asking you to fear a risk that is 80,000 times smaller than the risk they're helping you ignore.
I take 10,000–20,000 IU daily, because I do not want to experience the consequences of chronic deficiency over decades. I am legally not allowed to sell you what I recommend or live by. And I would rather tell you that directly than pretend the RDA is anywhere near adequate.
The Biggest Gaps: Where RDAs Are Most Wrong
Vitamin D3 is the most dramatic example, but it is not the only nutrient where the gap between RDA and optimal is medically significant:
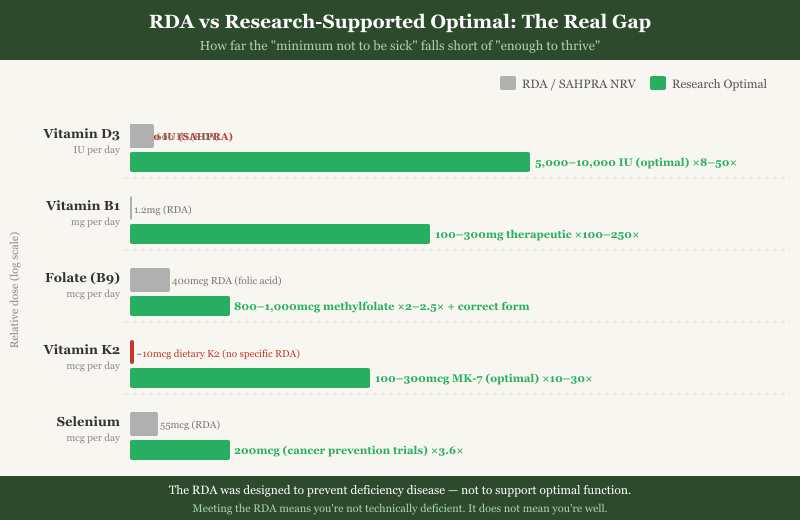
Vitamin D3 RDA: 600 IU. SAHPRA NRV: 1000 IU. Research-supported optimal: 5,000–10,000 IU daily for most adults. The gap is about 8 times, depending on which standard you use against which research benchmark.
Vitamin B1 (Thiamine) RDA: 1.1–1.2 mg/day. Subclinical deficiency is dramatically underdiagnosed — particularly in people consuming refined carbohydrates, alcohol, or taking metformin. B1 is the co-factor for pyruvate dehydrogenase (the enzyme that converts glucose to usable energy in neurons) and alpha-ketoglutarate dehydrogenase (a Krebs cycle enzyme). Subclinical B1 deficiency produces fatigue, depression, anxiety, poor concentration, and peripheral nerve pain. These are commonly treated with antidepressants and anxiolytics when the actual problem is a missing co-factor at 1 mg/day. High-dose B1 protocols (100–300 mg/day) have reversed fibromyalgia and autonomic neuropathy in documented case series. The RDA is 1 mg.
Folate (B9) and B12 The RDA does not distinguish between folic acid (the synthetic form in fortified foods and cheap supplements) and methylfolate (the biologically active form your cells actually use). Approximately 43% of the population carries MTHFR variants that significantly impair this conversion. For these individuals, the RDA for "vitamin B9" is actively misleading — they can meet it with folic acid and still be functionally deficient in the form their methylation cycle requires. Supplementing the wrong form is not neutral; unmetabolised folic acid may interfere with natural folate function in genetically susceptible individuals. Similarly, cyanocobalamin (synthetic B12) is less bioavailable than methylcobalamin for many people, especially those with gut absorption issues.
Vitamin K2 The RDA for vitamin K does not distinguish between K1 (phylloquinone, primarily involved in blood clotting and found in leafy greens) and K2 (menaquinone, involved in directing calcium to bone and away from artery walls). Most people in the Western diet are severely K2-deficient. There is no specific RDA for K2 — it is lumped into a total vitamin K recommendation built around K1. The therapeutic range for K2 (MK-7 form) for cardiovascular and bone benefit is 100–300 mcg/day; most people get less than 10 mcg from diet.
Trace minerals: selenium, boron, zinc, chromium Selenium at the RDA (55 mcg) prevents Keshan disease. At 200 mcg it shows meaningful cancer risk reduction in intervention trials. Chromium at RDA prevents severe glucose intolerance; at 400+ mcg it shows clinically meaningful insulin sensitivity improvement in studies. Boron has no established RDA despite evidence for bone density, testosterone metabolism, and brain function. It has been ignored — not because evidence is lacking, but because it is inexpensive, unpatentable, and disrupts no pharmaceutical market.
What Temple Foods Does — and Doesn't — Do About This
I will not pretend Temple Foods products are optimal by the standard of what the research supports. Within the SAHPRA OTC framework, they cannot be. What I can tell you is they are dosed as close to the legal ceiling as possible, using the correct forms: methylated B vitamins, D3 with K2-MK7 (not D2 and not K1), methylcobalamin (not cyanocobalamin), methylfolate (not folic acid). No silicon dioxide. No titanium dioxide. No magnesium stearate.
That matters. The form is often more important than the dose. But it is still not enough to correct a severe deficiency fast.
If you want to approach research-supported optimal D3 levels using OTC supplements in South Africa, the practical answer is taking multiple capsules daily. More costly. More inconvenient. The only legally available mechanism until SAHPRA reconsiders a framework that is actively harming public health.
I would prefer to make a 8,000 IU D3 capsule with full cofactor support. The regulatory environment does not permit it. So we formulate within the system, tell you the truth about what the system is, and let you make informed decisions from there.
What You Can Actually Do
Given that the RDA system is not your friend and that the South African regulatory environment is particularly limiting, here is what the evidence supports for anyone serious about optimising rather than merely surviving:
Test before you guess. A 25-OH vitamin D blood test costs less than R300 at most pathology labs. Know your actual level before picking a dose. Optimal is 80–110 nmol/L. Most indoor-living South Africans test at 40–60 nmol/L. If you're at 40, supplementing at the RDA will not move you into optimal range within a year.
Always supplement multiple nutrients together. Never take D3 alone — always with K2-MK7 (100–200 mcg) and magnesium (300–400 mg/day minimum, glycinate or malate form). Never supplement B vitamins in isolation — isolated high-dose single B vitamins can deplete related B vitamins through competitive pathway pressure.
Insist on correct forms. Methylfolate not folic acid. Methylcobalamin not cyanocobalamin. D3 not D2. K2-MK7 not K1. Magnesium glycinate or malate not oxide. The form matters more than the dose in several of these cases.
Start low, add cofactors, titrate up. Starting D3 at 1,000 IU and increasing to 5,000 IU over 4–6 weeks, with magnesium added simultaneously, prevents the cofactor-depletion symptoms people misattribute to toxicity. You're not being poisoned. You're healing faster than your micronutrient reserves can keep up with.
Reframe the risk question. The question is not "is this supplement safe at high doses?" The question is: what is the cost of chronic subclinical deficiency? Depression from B1 insufficiency. Cardiovascular calcification from K2 deficiency. Cognitive decline from D3 deficiency. These don't kill you tomorrow — they degrade your quality of life across years, quietly, attributed to ageing or stress or genetics, never to a correctable nutritional gap.
Frequently Asked Questions
Is the RDA the same as the NRV in South Africa?
Functionally, yes. NRV (Nutrient Reference Value) is the South African regulatory equivalent of the RDA — both are designed to establish the minimum intake required to prevent classic deficiency diseases in healthy populations. The SAHPRA NRV goes further by serving as the basis for OTC supplement dose limits, which is where the South African system becomes uniquely restrictive.
If the RDA is wrong, why do doctors still use it?
Doctors are trained within a system, and that system's reference texts are built around RDA-based standards. Most medical education in South Africa includes four to eight hours of formal nutrition training across a six-year degree. Doctors aren't deceiving you — they're well-intentioned people trained within a framework that was built by institutions with structural conflicts of interest they were never taught to question. The system, not the doctors, is broken.
Can I get vitamin D toxicity from high-dose supplements?
Technically yes, but the threshold is dramatically higher than most people are led to believe. Documented toxicity cases involve sustained use of 40,000–100,000+ IU daily for months. The Endocrine Society's formal position is that 10,000 IU daily is safe for long-term adult use. If you experience symptoms while taking 5,000–10,000 IU that you attribute to D3 — muscle cramps, palpitations, fatigue — the most likely cause is magnesium depletion from D3 increasing its demand. Add magnesium and reassess before stopping D3.
What is MTHFR and why does it matter for B vitamins?
MTHFR is a gene that produces the enzyme methylenetetrahydrofolate reductase — responsible for converting folic acid to its active form (methylfolate), which the methylation cycle uses. Approximately 25% of people have reduced-function MTHFR variants. For these individuals, meeting the folate RDA with folic acid is insufficient — they can consume adequate folic acid and still be functionally unable to produce enough active methylfolate. The fix is supplementing the active methylated form, not folic acid. The RDA framework doesn't distinguish between forms. SAHPRA's NRV system doesn't distinguish. Your cells notice the difference.
Why doesn't Temple Foods make higher-dose products?
SAHPRA does not permit OTC supplements to exceed NRV-based dose limits without classification as a scheduled medicine. A higher-dose D3 product would require a prescription pathway, removing it from the supplement market entirely. We formulate as close to the regulatory ceiling as legally possible, using the most bioavailable forms available. This is a regulatory constraint, not a formulation choice. We'd make better products if the framework allowed it.
Where do I start if I know nothing about my current levels?
Get a 25-OH vitamin D blood test — it's inexpensive and foundational. Then start magnesium glycinate (300 mg/day), a methylated B-complex, and D3+K2 at the maximum OTC dose available. After 90 days, retest your D3. If still below 80 nmol/L, discuss a supervised high-dose protocol with a functional medicine practitioner or integrative GP. The goal is evidence, not guesswork.
The Ice Cream Standard — Revisited
We started with ice cream, and we will end there — because the analogy holds perfectly at the close.
The minimum legal standard for ice cream doesn't tell you what good ice cream is. It tells you what isn't required to be called something else. You can comply with the standard and produce something that is essentially low-grade frozen junk in a nice container. It's legal. It's not good.
The RDA tells you what isn't a deficiency disease. It doesn't tell you what health is. You can meet the RDA for every nutrient in existence and still have subclinical thiamine deficiency making your brain foggy, subclinical D3 deficiency suppressing your immune system, subclinical K2 deficiency slowly calcifying your arteries, and subclinical magnesium deficiency creating the perfect conditions for insulin resistance. None of this shows up on a standard annual blood panel. None of it is what your GP is trained to look for. All of it is technically "normal" within the RDA framework.
The easiest, cheapest solution to many chronic health complaints is correct micronutrient supplementation at research-supported doses. That solution threatens no pharmaceutical market. It requires no prescription, no doctor visit, no long-term medication dependency. So the system doesn't teach it, doesn't validate it, and — through SAHPRA — actively limits access to it.
This is not conspiracy. This is economics applied to public health, with predictable outcomes for the people whose health is being managed.
Good ice cream is worth finding. So is actual health. They both require going beyond the minimum legal standard to get there.
Scientific References
Mialon M, Swinburn B (2020). Conflicts of interest of the 2020 Dietary Guidelines Advisory Committee. PLOS Medicine. PMC10966930
Holick MF et al. (2011). Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. Journal of Clinical Endocrinology & Metabolism, 96(7):1911–30. PMID: 21646368
Marcinowska-Suchowierska E et al. (2018). Vitamin D toxicity — a clinical perspective. Frontiers in Endocrinology, 9:550. PMID: 30294301
Whitfield KC et al. (2018). Thiamine deficiency disorders: diagnosis, prevalence, and a roadmap for global control programs. Annals of the New York Academy of Sciences, 1430(1):3–43. PMID: 30151974
Wan L et al. (2018). MTHFR C677T polymorphism and cognitive impairment. Molecular Neurobiology, 55(6):4905–4917. PMID: 28730451
Schurgers LJ, Vermeer C (2000). Determination of phylloquinone and menaquinones in food. Haemostasis, 30(6):298–307. PMID: 11356998
Giovannucci E et al. (2006). 25-Hydroxyvitamin D and risk of myocardial infarction in men. Archives of Internal Medicine, 168(11):1174–80. PMID: 18541825
Rayman MP (2012). Selenium and human health. The Lancet, 379(9822):1256–68. PMID: 22381456
Comments